Eosinofilos en Psoriasis
The likely Lilliputian meaning of eosinophils in psoriasis
DermWorld Insights and Inquiries
By Warren R. Heymann, MD, FAAD, August 1, 2026
Vol. 8, No. 8

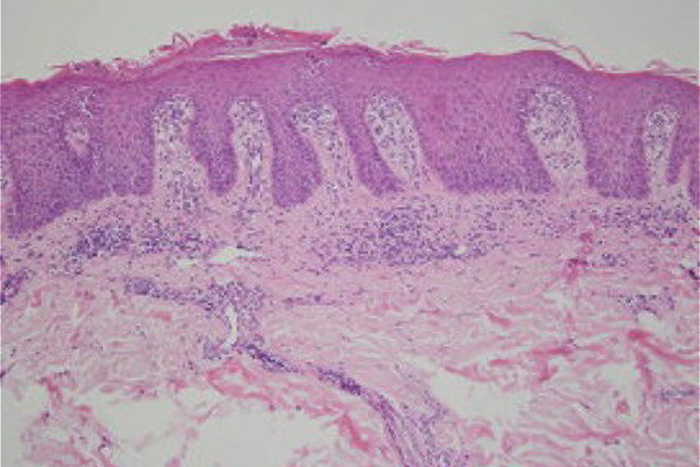
I will not berate myself for thinking that other disorders, such as a superimposed allergic contact dermatitis or drug eruption, could be responsible for disorders demonstrating eosinophils in a histologically psoriasiform eruption — indeed, this might be true in some cases. I was taught that eosinophils are not observed in psoriasis. Helwig reinforced this tenet in his classic 1958 manuscript, Pathology of Psoriasis. “The inflammatory cell infiltrate was of two types. One consisted of polymorphonuclear leukocytes. When present, it was located primarily on the tips of the papillae and served as the source of the leukocytes that migrated through the epidermis to form abscesses of Munro. The other consisted chiefly of lymphocytes and scattered monocytes and was located, for the most part, in the base of the papillae and the upper portion of the corium. Inflammatory cells were noted in neither the deeper corium or the subcutaneous fat. Plasma cells were rare, and eosinophilic leukocytes were absent (emphasis added). Mast cells usually were present but were not numerous.”(1)
The histologic presence of eosinophils is uncommon during physiologic conditions but is observed in various infectious, inflammatory, and neoplastic disorders. Caro-Chang and Fung classify the histologic presence of eosinophils into four categories: 1) Lesional eosinophils are highly characteristic such that, in their absence, the pathologist may question the diagnosis. These include arthropod bite reactions and scabies, urticarial dermatitis, and other eosinophilic dermatoses (bullous pemphigoid, Wells syndrome, others). 2) Lesional eosinophils are rare or absent, so that the pathologist may question the diagnosis in their presence. These include pityriasis lichenoides, graft-versus-host disease, and connective tissue disorders. 3) Lesional eosinophils are variable and — while in some cases, expected — are not required for diagnosis. These include drug reactions, atopic dermatitis, and allergic contact dermatitis. 4) Lesional eosinophils are variable and not expected but may be seen to a limited extent. These include lichen planus and psoriasis.(2)
“You should never be ashamed to admit you have been wrong. It only proves you are wiser today than yesterday.”
─ Jonathan Swift
Sanchez et al. believe that tissue eosinophilia in reputed eosinophil-poor dermatologic conditions presents a diagnostic pitfall, suggesting that tissue eosinophilia should not be used to rule out a diagnosis in these conditions.(3) What are the data for the presence of eosinophilia is psoriasis?
Rosa et al. observed eosinophils in 15 cases of 83 (18%) psoriatic patients. Of cases with eosinophils, none had more than three eosinophils upon examination of the entire dermis; there was no correlation with active treatment. The authors concluded that eosinophils are uncommon in psoriasis biopsies, and when present, they are found in small numbers.(4) Chau et al. observed dermal eosinophils in 25 of 51 (49%) psoriatic lesions, rarely observed in 24% (12/51), moderate in 18% (9/51), and dense in 8% (4/51).(5) Penn and Brinster noted the presence of eosinophils in 23 of 50 psoriasis specimens. There was no significant association between eosinophils and the degree of spongiosis.(6) Khalili et al. reported that eosinophils were present in approximately 70.3% of the 91 examined samples, with a mean eosinophil count of 2.42±0.63. Although there was no significant correlation observed between the clinical subtype and the average eosinophil count, eosinophils were most detected in the cases presenting generalized pustular psoriasis (100%) and vulgaris types (71.11%).(7)
Caro-Chang and Fung performed a systematic review of eosinophils and psoriasis in five studies that included 218 patients. The pooled prevalence of dermal eosinophils in psoriasis was 46%. The prevalences of one to five lesional eosinophils (24%) compared to >5 eosinophils (26%) were similar. There was no association between eosinophils and prior treatment. There was also no association between eosinophils and spongiosis. The authors suggest that although >5 eosinophils, as an isolated finding, would not be typical of psoriasis, it should not preclude its diagnosis without considering the overall histologic context.(8)
Why eosinophils are present in some psoriatic lesions is unclear. Interleukin-36 (IL-36), a potent proinflammatory cytokine that is a central driver of psoriasis, also promotes eosinophilic inflammation.(9) Biologics such as infliximab and brodalumab may cause peripheral eosinophilia.10 The precise meaning of eosinophils in psoriasis mandates further research.
In conclusion, dermatopathologists and clinicians must recognize that eosinophils may be observed histologically in psoriasis. If few in number, in keeping with the Jonathan Swift theme, their presence can be considered lilliputian and of little significance. Discontinuing medications may not be warranted. Alternatively, if tissue eosinophilia is prominent, a careful clinical assessment is appropriate. With further studies, recommendations will become more precise.
AAD Clinical Image Collection
View hundreds of images of dermatologic disease in all skin types and tones on the AAD Clinical Image Collection.
Point to Remember: Eosinophils may be observed histologically in psoriasis. If few in number, their presence is likely of little clinical significance.
Our expert’s viewpoint
Maxwell A. Fung, MD, FAAD
Professor of Clinical Dermatology and Pathology, UC Davis Department of Dermatology
Director, UC Davis Dermatopathology Service
On at least two levels, I found remarkable Dr. Heymann’s superb summary of a topic that I suspect might be regarded by some readers as esoteric or even trivial, that of eosinophils in psoriasis: First, because of the wide documented range of eosinophils in lesional psoriasis (18-73%). Second, because, just within the past eight years, at least eight original studies, including two systematic reviews, from investigators at seven different institutions in three different countries on opposite sides of the planet were all inspired to research this topic!
Both facts reflect broader realities that are largely referable to fundamental principles of formulating a good research question (acronym “FINER”(11)). These have helped me survive and occasionally thrive amidst the rigors of full-time academic dermatology and dermatopathology for the past quarter century.
Feasible: Research performed by busy clinicians devoting their lion’s share of effort to patient care tends to be conducted during evenings and weekends, with little-to-no protected time and little-to-no funds/grants. This reality seems prevalent among dermatopathologists and dovetails with the schedules and partly overlapping incentives of medical students and residents/fellows. A corollary is that there can be a premium on studies lacking significant expense and conducted as time permits.
I suspect eosinophils are appealing in this regard, since they are a free ancillary diagnostic “test,” being already included in the cost of preparing the H&E slide. Moreover, eosinophils are universally recognized, uncontroversial, and easy to definitively confirm or exclude by H&E alone (the challenge of eosinophil degranulation notwithstanding).
Interesting: This is ultimately subjective, but the multiple publications signal a de facto consensus of interest by multiple journal editors and reviewers. Certainly, clinicians and patients struggling to effectively manage patients whose biopsies show “psoriasiform spongiotic dermatitis” would be grateful for anything that might permit more specific histologic classification in the notoriously overlapping clinicopathologic spectrum of psoriasiform and spongiotic/eczematous changes that have, additionally, been demonstrated at the molecular level.
For the message that lesional eosinophils, especially in low numbers, are not against psoriasis, the dermatologist may retain (rather than exclude) the consideration for these patients a rich armamentarium of targeted anti-psoriatic therapies.
Novel: Dr. Heymann’s review documents that the concept of “no eosinophils” in psoriasis has been in the literature for two-thirds of a century (since 1958). In the absence of new or novel data, dermatopathologists have relied on anecdotal statements from key opinion leaders that went reasonably unchallenged in textbooks (edition after profitable edition) and taught to generations of trainees. In a field devoid of prospective studies, essentially all data is biased, being derived from cases biopsied in clinical practice, i.e., chronic, severe, refractory, heavily treated, and/or atypical (e.g., superimposed contact dermatitis, eczematized psoriasis), often to rule out psoriasiform mycosis fungoides or to “confirm” psoriasis prior to initiating immunosuppressive therapy. Any and all of these factors might result in non-classic histopathologic features, such as eosinophils.
Did you know it was not until 2021 that consensus-based minimal diagnostic criteria for the clinical diagnosis of psoriasis vulgaris were published?(12) It is a testimony to the clinical distinctiveness of psoriasis and extant therapeutic success that dermatologists have “gotten away” with gestalt clinical diagnosis of psoriasis for so many decades!
My sense is that the wide range in lesional eosinophil prevalence (18-70%) is multifactorial but attributable to the lack of uniform inclusion criteria, compounded by differences in practice mix, and inability to control for confounding variables such as therapy. Differences in method of eosinophil assessment might account for minor differences. To date, no study has employed the 2021 consensus-based clinical criteria for case selection. For example, a 2025 study’s inclusion criterion was “clinical features of typical psoriasis,”(7) similar to that of most studies. So, while the differing results are novel in themselves, it likely reflects the inability to conduct strict case selection in a retrospective setting in the absence of a validated or objective clinical diagnostic gold standard.
Ethical: For all their limitations, retrospective studies tend to easily meet, if not be exempted from, the requirements for ethical research maintained by institutional review boards. This is a boon to legions of clinicians and trainees performing research on evenings and weekends. They also often represent the best available data in fields such as pathology for which prospective studies would be challenging if not prohibitive.
Relevant: Meaning clinically relevant, which is a more objective or practical requirement compared to the subjective requirement of being “interesting.” In addition to maximizing the availability of treatments, the conundrum of so-called “psoriasiform spongiotic dermatitis” as well as its commonly encountered differential diagnosis, “spongiotic dermatitis,” both seeming to be inflicted by dermatopathologists upon dermatologists with regularity, reflects a long-standing inability to reliably and accurately distinguish psoriasis from eczematous dermatitis, or to distinguish among the various forms of spongiotic/eczematous dermatitis. Any novel data that help confirm, or, in this case, avoid inappropriately excluding a diagnosis, will have clinical value.
In summary, in an era wherein cutting-edge diagnostic dermatopathology is focused on the latest immunostain or molecular assay, most histologic diagnoses worldwide continue to be established solely by vintage technology: light microscopic assessment of H&E stained tissue sections obtained from a paraffin embedded block of formalin fixed tissue. The recent uptick in attention to the status of eosinophils in psoriasis represents an international recognition of the interest, clinical relevance, and feasibility of unturning a few more of the last remaining H&E “stones.”
DermWorld Insights & Inquiries
The viewpoints expressed are my own and do not reflect those of my employer (University of California) or the American Society of Dermatopathology, for which I currently serve as president.
I am the senior author of references 2, 5, and 8.
No generative AI or AI-assisted technologies were employed in the writing process of this viewpoint. Organic intelligence (OI) was solely employed.
References
Helwig EB. Pathology of psoriasis. Ann N Y Acad Sci. 1958 Nov 10;73(5):924-35. doi: 10.1111/j.1749-6632.1959.tb40869.x. PMID: 13627839.
Caro-Chang LA, Fung MA. The role of eosinophils in the differential diagnosis of inflammatory skin diseases. Hum Pathol. 2023 Oct;140:101-128. doi: 10.1016/j.humpath.2023.03.017. Epub 2023 Mar 30. PMID: 37003367.
Sanchez I, Ibraheim MK, Lee BA, Kraus CN, Elsensohn A. Eosinophils in Traditionally Noneosinophil-Rich Dermatoses. Am J Dermatopathol. 2023 Dec 1;45(12):820-821. doi: 10.1097/DAD.0000000000002550. PMID: 37883982.
Rosa G, Fernandez AP, Schneider S, Billings SD. Eosinophils are rare in biopsy specimens of psoriasis vulgaris. J Cutan Pathol. 2017 Dec;44(12):1027-1032. doi: 10.1111/cup.13042. Epub 2017 Oct 13. PMID: 28901561.
Chau T, Parsi KK, Ogawa T, Kiuru M, Konia T, Li CS, Fung MA. Psoriasis or not? Review of 51 clinically confirmed cases reveals an expanded histopathologic spectrum of psoriasis. J Cutan Pathol. 2017 Dec;44(12):1018-1026. doi: 10.1111/cup.13033. Epub 2017 Sep 15. PMID: 28833447.
Penn L, Brinster NK. Eosinophils Among the Histological Features of Psoriasis. Am J Dermatopathol. 2019 May;41(5):347-349. doi: 10.1097/DAD.0000000000001303. PMID: 30422830.
Khalili M, Kooshesh A, Shamsi-Meymandi S, Mehrolhasani N, Amiri R, Rezaei Zadeh Rukerd M, Aflatoonian M. Exploring the Significance of Eosinophil Infiltration in Diagnosis of Psoriasis: A Cross-sectional Analysis. Iran J Pathol. 2025;20(1):18-23. doi: 10.30699/ijp.2024.2013501.3191. Epub 2025 Jan 10. PMID: 40060237; PMCID: PMC11887645.
Caro-Chang LA, Fung MA. Eosinophils in psoriasis: A systematic review and meta-analysis introducing a study quality assessment tool for diagnostic pathology studies. J Cutan Pathol. 2024 Jun;51(6):441-449. doi: 10.1111/cup.14604. Epub 2024 Feb 28. PMID: 38415867.
Zhang WR, Bhutani T, Schulman JM, North JP. The association of interleukin-36 staining intensity with histopathologic findings of eosinophil count and spongiosis in patients with psoriasis: A secondary analysis of a retrospective immunohistochemical and chart review pilot study. J Cutan Pathol. 2025 Apr;52(4):251-253. doi: 10.1111/cup.14711. Epub 2024 Aug 31. PMID: 39215601.
Sugiura R, Terui H, Shimada-Omori R, Yamazaki E, Tsuchiyama K, Takahashi T, Aiba S, Yamasaki K. Biologics modulate antinuclear antibodies, immunoglobulin E, and eosinophil counts in psoriasis patients. J Dermatol. 2021 Nov;48(11):1739-1744. doi: 10.1111/1346-8138.16102. Epub 2021 Aug 8. PMID: 34368997.
Cummings SR, Browner WS, Hulley SB. Conceiving the research question and developing the study plan Designing Clinical Research. 2013 4th ed Philadelphia Lippincott Williams and Wilkins:14–22.
Abo-Tabik M, Parisi R, Willis SC, Griffiths CEM, Ashcroft DM; Global Psoriasis Atlas (GPA). Development of clinical diagnostic criteria for chronic plaque psoriasis: an international e-Delphi study. Br J Dermatol. 2021 Aug;185(2):455-456. doi: 10.1111/bjd.20096. Epub 2021 May 31. PMID: 33811321.
posted by dermatica at
August 10, 2026
|
0 Comments
![]()
![]()
